Welcome to Impact Factor. I'm Perry Wilson. This week: Aspirin for primary prevention is dead.
We shall not look upon his like again.
Only a touch of hyperbole here, as the results of the ASPREE trial flip everything we thought we knew about aspirin on its head and draw to a close a rough month for the willow bark–derived compound.
Some quick background: We've had data for decades that aspirin can prevent recurrent heart attacks and strokes—secondary prevention. And up until recently, mixed data leaned toward a benefit for primary prevention as well. The meta-analyses on this topic even suggested that there might be a benefit in terms of all-cause mortality and, tantalizingly, a reduction in the risk for colon cancer if you take aspirin.
Then everything changed.
Two weeks ago, we were treated to the results of the ASCEND trial, which looked at aspirin for primary prevention in 15,000 patients with diabetes.
ASCEND Study Collaborative Group. Effects of aspirin for primary prevention in persons with diabetes mellitus. N Engl J Med. Epub 2018 Aug 26. Source Accessed September 17, 2018
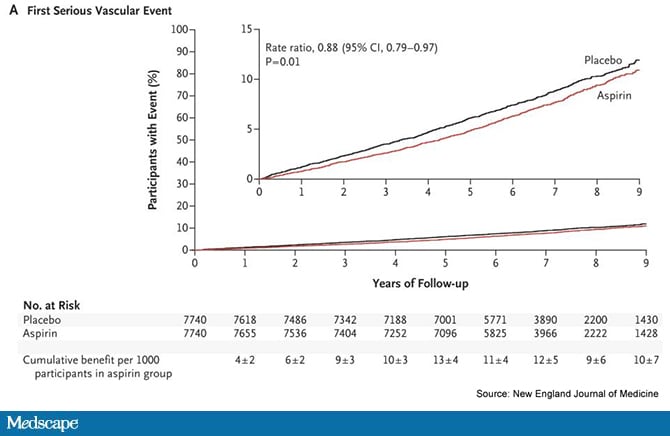
While there was a modest benefit in terms of reduction in cardiovascular events, a fairly significant increase in the risk for major hemorrhage took the wind out of the sails of those results. Strike one.
Strike two was the ARRIVE study, a randomized trial of 13,000 patients with moderate cardiovascular risk. Aspirin had no effect on all-cause death or the cardiovascular outcome.
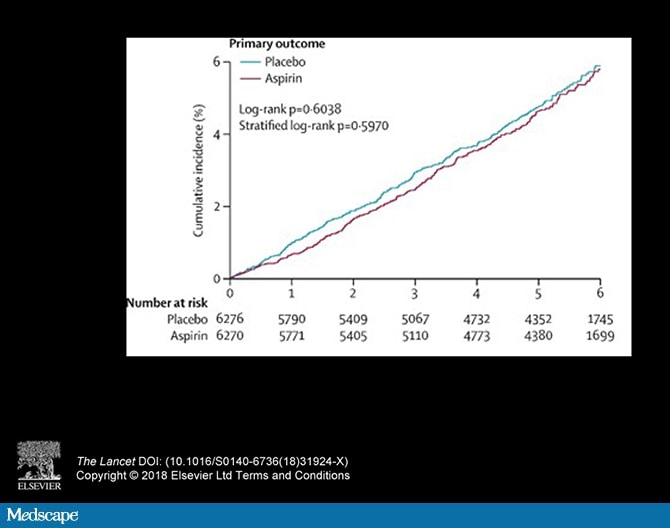
Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. Epub 2018 Aug 26. Abstract
And now, strike three comes in the form of a trio of papers published in the New England Journal of Medicine, examining the results of the ASPREE trial. These studies paint an even bleaker picture for aspirin.
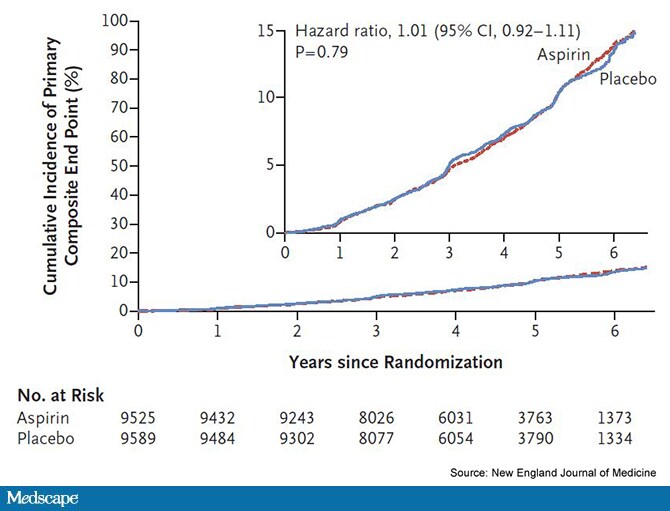
The ASPREE trial was a huge study, enrolling almost 20,000 individuals in the United States and Australia. It was targeted to older adults—over age 70—a group expected to be at higher risk for cardiovascular disease or death. The primary outcome was a composite of death, dementia, and disability, an effort to capture the fact that in an older population, simply living longer is not always the only goal.
McNeil JJ, Woods RL, Nelson MR, et al. Effect of aspirin on disability-free survival in the healthy elderly. N Engl J Med. Epub 2018 Sep 16. Source Accessed September 17, 2018
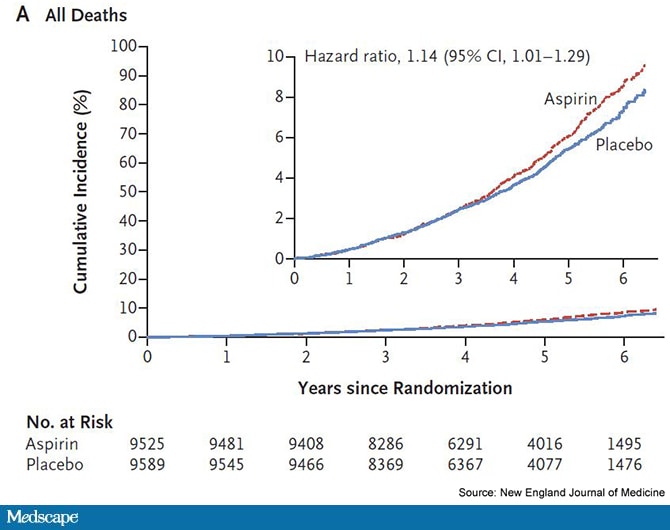
Aspirin had no effect on the primary outcome. But the results get weirder. Looking just at all-cause mortality, the rate was higher in the aspirin than the placebo group.
McNeil JJ, Woods RL, Nelson MR, et al. Effect of aspirin on disability-free survival in the healthy elderly. N Engl J Med. Epub 2018 Sep 16. Source Accessed September 17, 2018
Fortunately, absolute mortality rates were really low. It would suggest that for every 100 patients you treat with aspirin, you'll see one extra death over a 5-year period. This is tiny, but still, this is aspirin. What happened to the wonder drug?
Spurred on by these strange findings, the authors published their second paper in the journal, examining the causes of death. And the findings were driven by—wait for it—cancer.

McNeil JJ, Nelson MR, Woods RL, et al. Effect of aspirin on all-cause mortality in the healthy elderly. N Engl J Med. Epub 2018 Sep 16. Source
This is where we'd insert a record scratch if Impact Factor weren't such a sophisticated production.
The rate of new cancer diagnoses and death from cancer was higher among those taking aspirin compared with those on placebo. This runs counter to much of what we've been told about aspirin in the past.
What's going on? I suspect... nothing. And here's why.
Death was not the primary outcome in the ASPREE trial. We specify a primary outcome because we know that the more outcomes we test, the higher the chance we'll see a false positive. In fact, if you account for multiple comparisons in the ASPREE study, the "death signal" would not have achieved statistical significance. We would chalk it up to simple noise in the data.
Nevertheless, now we go down this rabbit hole and try to explain why death is higher. And what you have to realize here is that if we got a skew in death rates by chance alone, something would have to explain it; everyone dies of something. So the finding that it was "cancer" is not necessarily that weird either.
My number-one rule in medical research goes like this: One study doesn't prove anything. One study can suggest. One study can raise doubts, but one study never proves. So let's not jump on the aspirin-causes-cancer train. Too many prior studies conflict with that finding.
What we do have here, though, are multiple studies, in multiple moderate-risk populations, that all reach the same conclusion. Aspirin has no role in the primary prevention of heart disease.
Has something changed? Actually, yes. We are way, way better at preventing heart disease than we ever were in the past. We treat cholesterol and blood pressure more aggressively, and we manage diabetes much better.
In fact, all three of these trials share one other point in common (aside from the fact that they found that aspirin did essentially bupkis). They all dramatically overestimated the cardiovascular event rates they would see.

Our old risk equations aren't that good anymore, because we are doing a better job at reducing risk. And in this brave new world, aspirin appears to have lost its mojo.
So, aspirin, my old friend: Good night, sweet prince, and flights of platelets sing thee to thy rest.
Medscape © 2018 WebMD, LLC
Any views expressed above are the author's own and do not necessarily reflect the views of WebMD or Medscape.
Cite this: Strike Three for Aspirin in Primary Prevention - Medscape - Sep 17, 2018.










Comments